
We believe health equity is the foundation of quality. Given that high quality patient care is at the center of our mission, the pursuit of health equity must form the basis of our work. We need to discover the impact of race on access to care, treatments, clinical outcomes and patient experiences. Where inequities are identified, we must understand them at their root cause and commit to the countermeasures that create highest quality clinical outcomes for all. To do so, we will:
• Establish health equity as a “mission critical” element of our quality work.
• Eliminate inequities in clinical care.
• Reduce social barriers to a healthy life through population health management.
Addressing Health Care Disparities during COVID-19
In the United States
The COVID-19 pandemic in the U.S. has disproportionately affected African Americans, Latinx and Native Americans not only in terms of the incidence of disease but also in terms of mortality. In the U.S., African Americans have a 3.5 times higher age adjusted mortality compared to whites. Latinx and Native Americans have 2.5 times higher age adjusted mortality compared to whites.
At DUHS
In our renewed commitment to our community to identify, measure and eradicate health inequities, we examined our first six month experience with managing patients with COVID infections serious enough to warrant admission to a Duke Health hospital. In that period, we observed:
- 67 percent of those hospitalized and discharged were people of color, while 28 percent were white, consistent with the disproportionate burden of serious illness that has affected people of color in our community and across our country. 40 percent were African American while 27 percent were Latinx.
- The in-hospital mortality rate was 18 percent for whites, 12 percent for African Americans, and 6 percent for Latinx, and these trends persisted when mortality rates were adjusted for age.
- In addition, rates with which disease modifying treatments with Remdesivir were used were similar among the three groups (whites 21 percent, African Americans 20 percent and Latinx 30 percent). So too, rates with which life-saving treatments with Decadron were used were similar by race (whites 21 percent, African Americans 22 percent, Latinx 24 percent).
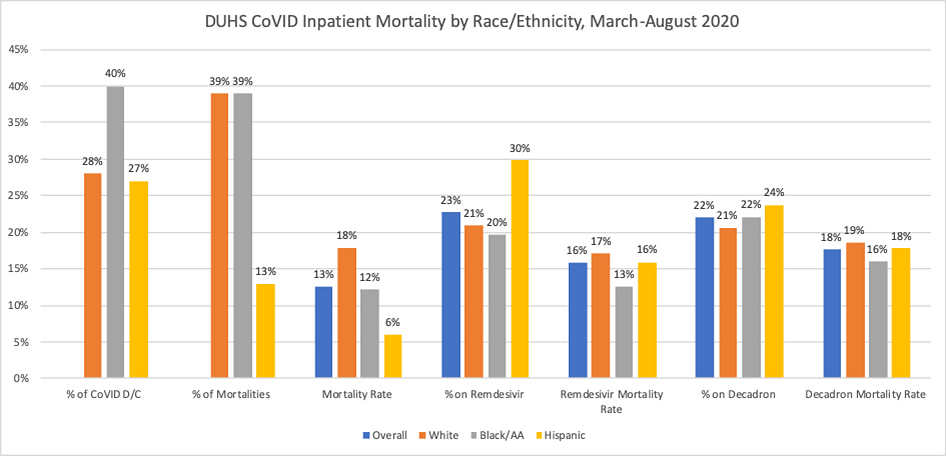
These data suggest that people of color in our community did disproportionately experience a higher rate of serious COVID illness requiring hospitalization, but there were no disparities in in-hospital mortality or in the use of COVID specific therapies among whites, African Americans, or Latinx patients treated at Duke. The mortality outcomes stand in contrast to what has been reported nationally.
At Duke, we take seriously the moral imperative to provide excellent care for all and work daily to live up to those values. We commit to transparency in our outcomes and to address inequities where we find them. We also recognized that the outcome of seriously ill and hospitalized patients is only part of the story when it comes to understanding the full impact of the pandemic on people of color but we are grateful for the opportunity to serve well those in greatest need. We also recognize that we have work to do to be more welcoming and accessible to all in need.
Addressing Disparities in Women's Health Care
At Duke Health, we recognize the impact of systemic racism and bigotry in women’s healthcare that we experience in our state and nation and have a long-held commitment to eradicating these disparities as one of the most important missions in our care of patients.
Black women are three times more likely to die in childbirth than white women; this disparity is not fully explained by differences in health status, socio-economic status or patterns of healthcare use. Therefore, it is imperative that we examine ourselves as part of the healthcare system and the structural racism entrenched within that system. We have a duty to diligently combat racism and bigotry with creative and consistent efforts that include our entire team.
In response:
- We will provide opportunities for all Duke Ob/Gyn team members to be trained in implicit bias, bystander skills and cultural competency.
- We will consistently evaluate our policies, practices and outcomes to identify and eradicate inequities for our patients and our team members.
- We will consistently assess our work culture and learning environment to ensure that all members of our team — staff, trainees, and faculty — have the opportunity to thrive and advance their individual careers while contributing to the realization of our Duke OB/Gyn mission, vision and values.
- We will continue to support our patients and our community through our clinical, educational and research efforts, as well as through philanthropy and volunteerism.
- We will listen and thoughtfully respond to feedback, concerns and criticisms from our patients, our community and our team members.
- We will be steadfast, unwavering and unrelenting in our pursuit of racial justice and equality.
Resources
Duke University is proudly home to the Duke Center for Research to Advance Healthcare Equity (REACH), one of 12 centers funded by the National Institute of Minority Health and Health Disparities (NIMHD), part of the National Institutes of Health. These specialized research centers are designed to conduct multidisciplinary research, research training, and community engagement activities focused on improving minority health and reducing health disparities.


